

Canada and Australia combine to show structural corruption and incompetence.
Simple, global aviation structure
Commercial aviation is a fairly standardised, top-down product. This is a strength and a weakness. In simple terms, it is structured globally like this:
International aviation triumvirate: ICAO; IATA; IFALPA
It is adequate to say that global aviation is run by a triumvirate comprising:
- International Civil Aviation Organisation ICAO
- International Air Transport Association IATA
- International Federation of Air Line Pilots’ Associations IFALPA

International Civil Aviation Organisation is to be considered, in simple terms, the global co-ordinating body and the source of regulatory standards. Covid-19 aviation policy has been co-ordinated at the ICAO level via ICAO’s Council Aviation Recovery Task Force CART guidance material, which has top-down influence on ICAO member states’ Covid policy. ICAO is not absolutely definitive, but is highly influential.

International Air Transport Association is effectively a global trade body for air transport that brings together and represents companies. It is key in policy implementation across corporations. It has been instrumental in Digital ID development and deployment within travel. As such, it incorporates, allies and contracts with broad spectrum commercial and corporate service providers. Its current head, Willie Walsh, was former CEO of IAG (umbrella airline group) and British Airways.

International Federation of Air Line Pilots’ Associations could be considered the global airline pilots’ umbrella union organisation. Globally, pilot union response to Covid-19 and resultant policy has been almost uniform and on the side of WHO/government/corporations and pro-gene therapy etc, with little to no regard for the obvious risk/threat issues of Covid-19 policy responses that were inherent and obvious. Minority membership views i.e. those minority groups of pilots who urged caution about gene therapy use in aviation, have not been represented or listened to by unions. The proof of this is in the inability and unwillingness of unions to resist gene therapy use, even when they were told there were strong medical, scientific, legal and regulatory reasons to exercise varying degrees of caution.
Power and control in aviation runs roughly thus:
- Manufacturers (Boeing, Airbus etc)
- Airlines
- Regulatory structure (ICAO, governments, national regulator)
- Labour unions
Arguably, power in aviation does not lie with a national (captured and mis-incentivised) regulator. It actually lies in the corporate lobby power and corporatocratic interests of the aircraft manufacturers and airlines. The regulators are a veneer of control and containment of that corporate power. Labour unions can be considered a control and containment mechanism of aviation labour, constrained by labour and employment law as well as their own leadership “views and priorities”.
If a regulator’s income derives directly from those it regulates, its regulatory interest and capability has been compromised. This is the standard regulatory income model across multiple countries, be it the FDA and MHRA, or the FAA and CAA. How can you bite the hand that feeds you?
There is a single, unassailable proof of my claim in the form of the 737 MAX, which proves several things:
- Boeing did what it wanted to the 737 airframe to make the MAX.
- While it looked like it conformed to aircraft design and operation regulations set by the FAA and EASA amongst others, it simply did not.
- Boeing lied to and misled the FAA and by extension, other regulators. The FAA and EASA were unable to regulate Boeing effectively at all because both granted airworthiness certificates to the 737 MAX, which then crashed twice and was shown to be deeply flawed. The FAA and other aviation regulators FAILED to regulate. Effective regulation would have prevented the crashes and the deaths.
- Any other regulator who granted their own airworthiness certificates to the 737 MAX were ultimately duped in the same way as the FAA and EASA.
- Even this wikipedia page tells you that other regulators:
- were, like Europe’s EASA, either duped like the FAA; or
- deferred to the FAA’s or another regulator’s certification process (while the UK was still in the EU, its Civil Aviation Authority deferred to EASA and FAA);
- lag the manufacturer. Only after the MAX crashes did the regulators find out what Boeing had done and how poor their regulatory processes and structures were. If there were no regulatory shortfalls, no changes to regulatory processes etc would have been necessary. Regulators like the FAA and EASA changed their processes after the crashes. That’s a flat out admission of historic incompetence at the least.
- Airlines either had no idea that the 737 MAX was so flawed, or they chose to operate them knowing that they were, and they relied on pilots to save the day from flaws that beat two human crews both times. This isn’t a good position for airlines to have to admit being in. If they didn’t know then they didn’t have the independent technical capability to identify deep flaws in a product they bought in droves. If they did know then they chose to tolerate those flaws. Airlines never led the curve on the MAX. They just breathed a sigh of relief that they weren’t Lion Air or Ethiopian Airways, then they bit the bullet as their MAX fleets were grounded.
The above, I believe, allows me to suggest to you the following:
Any assumption you have about competence, sufficient power and capability, and correctly incentivised active involvement of regulators in aviation is likely wrong. We don’t know what we don’t know and it takes certain rare events to open Pandora’s box or to peek behind the wizard’s curtain, to then realise that our assumptions are unproven until tested.
Unions simply do not figure
Pilot unions were absolutely nowhere on this matter. They simply do not meaningfully figure in bleeding edge, pro-active regulation. They will tell you they do, but the MAX proves that they don’t. If you don’t have a hand in the certification of and your members’ operation of a killer airframe, anything you actually are involved in is small beer by comparison. It is a mistake to believe otherwise. Unions run around after the fact, dealing with scraps thrown from the manufacturers’, airlines’ and regulators’ tables, in that order. Unions like to feel and want others (especially their members) to believe that they have a deserved and self-earned seat at the table. They don’t. Those seats belong to someone else and sometimes the owners invite unions to sit in them when it is convenient, makes for good optics and/or secures their corporate objectives.
Covid in aviation is an exact analogue of the 737 MAX, played out globally. Essentially, aviation actors have fallen for the same kinds of tricks in Covid as they fell for in the MAX. Some of the actors know it, some might not. None of them are going to openly admit to either being wrong, being duped or complicit even when they are looking at incidents and accidents that are causally tied to their own decisions and actions.
Why?
Because to do so is to admit that aviation isn’t safe because “we at the top levels of it are either incompetent, wrongly incentivised or unsafe ourselves.”


Aviation in a time of Covid
Take the above context and apply it to the following examples of aviation regulation in a time of Covid.
Instead of the certification of aircraft being “fit to fly”, as in the 737 MAX, let’s turn our gaze to the certification of pilots being fit to fly.
What a vaccine mandate in transport and/or society means
Mandates guarantee one thing, above all else.
They guarantee that a nation’s entire population is forced into a single medical paradigm and therefore the whole population is exposed to the same types and degrees of risk, which includes:
- risk of being wrong;
- risk of impartial knowledge at the time the mandate forces irreversible actions;
- risk of unforeseen consequences;
- risk of compounded errors and double-down mentalities in those who made the decisions and even in the compliant population;
- risk that emotions override rational thought into the future, which can prevent policy changes and redress for errors etc.
Canada
Canada implemented “no jab, no job” mandates across the widest spectrum in the Western world, including the lock out from transportation of unvaccinated citizens. These insane, unjustified policies are still in place: masks are ongoing; travel mandates may have another month to run (damage is already done); vaccine apartheid remains rife.
Canada’s transportation regulator, Transport Canada TC, blindly supported the mandates and use of gene therapies in pilots and air traffic controllers. In no way did it exercise caution, seek to maintain a control group or check back against its own principles of aviation medical safety.
An egregious example of this is back in July 2021 when TC faced challenges and questions around its long-standing rule that Canadian pilots and ATCOs were not allowed to engage in medical trials. Faced with that stopper, Transport Canada simply deleted the rule. You can see a quick lay out of this here, courtesy of the Global Aviation Advocacy Coalition’s article (quick read):

People have argued and still do argue that Covid gene therapies aren’t in trial, have been fully tested and are fully approved. This was and still is woefully wrong. I have never encountered someone arguing completed testing and full approval who could prove it, because the proof doesn’t exist.
EUA/CMA and Canadian Interim Authorisations are not full approval. Phase 3 clinical trials for these products are all still running and have been shown to be badly designed, badly run, possibly fraudulent and very limited. Sources to check all this are
and in the relevant regulatory webpages for each gene therapy. The easiest to navigate to find EMA/CMA documentation are MHRA, EMA and FDA. Canada’s are trickier. The documents clearly state the kinds of testing that were curtailed or excluded or exempted. Those areas of testing are all the ones that are increasingly problematic for those who took the gene therapies but correlation does not equal causation, and never does if you don’t investigate a possible link.
So, the above is an example illustrating that:
- For some reason(s) not fully understood or explained, Transport Canada made an executive decision to mandate and thereby affect all pilots and ATCOs it regulated, without any effective consultation with the people affected.
- Its decision directly resulted in all of those people being forced into a single medical paradigm. Now, 100% of the people in the Canadian flying industry are irreversibly dosed. The ones who aren’t are out of the business and in a tiny minority. There is no safety buffer and no control group.
- The aviation regulator acted irresponsibly, possibly criminally. If it encouraged and allowed anyone it regulated to engage in, directly or indirectly, medical trials and/or use products still in medical trial, while its rule against doing so was still in force, it is liable. Also, those individuals who took those products while that rule was still in force have broken that rule. That’s possibly criminal if they engaged in flight operations under their certificates and licences.
Canada’s decisions are individual and arbitrary. They do not relate to how other ICAO nations have regulated aviation, nor do they relate to science or medical research. They may have similarities to other nations but they show that Canada was able to set its own internal aviation regulatory policy that, as you will see from the following Australian example, is not bound or constrained entirely by ICAO guidance.
Australia
Australia is likely equal first or very close second to Canada when it comes to Covid policy in transportation and wider social impact.
Largely, what I describe above for Canada has equivalence in Australia.
However, in Australia there is a face and a name. There’s a trail of public video statements that aren’t going away, which should trigger concern in anyone who watches them.
In July 2021, Australia’s Civil Aviation Safety Authority CASA appointed Dr. Kate Manderson and Dr. Tony Hochberg as Principal and Deputy Principal Medical Officers, respectively.
By July 2021 there was already a wealth of research into Covid risk versus gene therapy risk illustrating that, for anyone under 65 years old (working pilots), risk from Covid was known to be extremely low (Covid infection fatality ratio below 0.15%). It was already known that language, definition and classification subversions were driving false pandemic data, as well as testing tool and strategy flaws doing the same. There was already analysis that showed gene therapy efficacy was, based on Pfizer’s published trial data, sub 1% on an absolute risk reduction basis, for the healthy people that Pfizer had and still is testing it on. No testing was done on anyone who was unhealthy, pregnant etc.
By October 2021, there was even more evidence that the mainstream narrative was faulty and that the gene therapies had deleterious effects on human health. There was no basis to claim with certainty that they were “safe and effective”. At best, any responsible and knowledgeable medical professional should have given a nuanced or conditional response based on the current research and evidence base.
In simple terms, all drugs have risk and none are “safe”.
In respect of Covid gene therapies, no matter how many doses have been delivered, there is no analogue for the passage of time and there is no knowledge of the long term effects of these products on the human race. Despite this unassailable fact, in October 2021 and then Jan 2022, Dr. Manderson appeared in two video streams with Aircraft Owners and Pilots Association of Australia AOPA (below), in which she expressly stated that she and CASA encouraged all pilots to be dosed.
She also stated with certainty that gene therapies were “safe and effective”. She also admitted that the gene therapies did cause myocarditis and pericarditis in some people. She presented no evidence base or references for her or CASA’s opinions, stance or policy.
Dr. Manderson was still willing to say she and CASA were happy about these products’ use in aviation “in the long term”, in specific relation to the myocarditis and pericarditis they trigger. Both of those conditions can have permanent long term deleterious effects on humans even after they are considered to have recovered. This is reflected within ICAO’s own Manual of Civil Aviation Medicine (Doc 8984).
If a medical intervention is known to have a risk of VITT, CVST, myocarditis, pericarditis etc, it is not “safe”. If one does not know why or in whom these conditions may occur, one’s knowledge about the intervention’s mechanism of action is incomplete. No one is able to predict accurately who in the general populace will suffer vaccine-induced severe adverse events (SAE) or fatalities, or say exactly why. It is now formally recognised that Guillain-Barré Syndrome is caused by at least one of the Covid gene therapies, when previously this had been ignored and denied. Why it occurs has not been fully explained.
Further, Dr. Manderson was also recorded directly addressing commercial pilots, where she repeated the same messages with no justification or evidence and again encouraged that they all be dosed without nuance or conditionality.
CASA and Dr. Manderson have refused to answer any queries sent to them regarding Covid gene therapy safety issues.
Even in the face of multiple, recent international and Australian public enquiries directed at the CASA board and Dr. Manderson – comprising 11 specific questions (above) regarding Dr. Manderson’s statements about Covid gene therapy safety, myocarditis and pericarditis – CASA and Dr. Manderson stonewalled those enquiries with a contemptuous, nonsensical and irrelevant reply, which was copied off the CASA website. CASA’s use of the following statement exposes, yet again, serious shortcomings in aviation regulation:
“The International Civil Aviation Organization endorses vaccination against COVID-19 as a core element of a multi-layer risk management strategy for aviation safety and international air transport. This includes vaccination of aviation personnel. For more information, see the COVID-19 vaccination fact sheet on our website.”
In no way does what ICAO “endorse” form a complete justification for what an ICAO nation state such as Australia must implement as policy. ICAO does not have demonstrably independent, peer-reviewed published analysis of Covid gene therapy risk benefits. Some of its briefing/analysis documents are inadequate even to lay people.
Here are examples of what ICAO has said to date:
(Excepts from) Joint Statement on prioritization of COVID-19 vaccination for seafarers and aircrew 25 March 2021
“Maritime and air transport rely on seafarers and aircrew. They are key workers required to travel across borders at all times, which may result in the need for them to present proof of a COVID-19 vaccination as a condition for entry in some countries. This is despite WHO recommendation that, at the present time, countries should not introduce requirements of proof of vaccination for international travel as a condition of entry, as there are still critical unknowns regarding the efficacy of vaccination in reducing transmission and limited availability of vaccines. For shipping and air transport to continue to operate safely, the safe cross border movement of seafarers and aircrew must be facilitated. We reiterate our call upon countries that have not done so to designate seafarers and aircrew as key workers.
Seafarers and aircrew need to be protected through vaccination as soon as possible to facilitate their safe movement across borders.
Our organizations fully support the timely development of an international harmonized framework for vaccination certificates, to facilitate international travel for seafarers and aircrew.”
ICAO ILO IMO WHO IOM Joint Statement
Bolded sections constitute a clear conflict partially ameliorated by careful phrasing. ICAO recognised in March 2021 “critical unknowns regarding the efficacy of vaccination in reducing transmission” yet it also believed “aircrew need to be protected through vaccination as soon as possible to facilitate their safe movement across borders.”
The critical unknowns of the gene therapies’ effects on transmission are inherently tied to:
- knowledge of their mechanism of action i.e. how they work in vivo and what effects they have individually that ultimately manifest as an effect on widescale transmission;
- risk benefit – if they don’t stop transmission at all but have other negative effects, risk benefit calculation is impacted.
ICAO was admitting that there was incomplete knowledge of these gene therapies but it deliberately stopped short of including “unknown short, medium and long term side effects”, which is unlikely to be an accidental omission because it is an inherent logical corollary of admitting that gene therapy effects (on transmission) are unknown.
This admission is in direct conflict with the belief that crew needed to be protected by Covid gene therapies in order to cross borders. In many, many ways this doesn’t stand up to reason. If transmission impact is unknown, you could vaccinate crews and they could still transmit. This is actually the case in the real world, so ICAO’s belief here is rubbished from the outset. ICAO’s belief is based on an assumption of total efficacy and safety, which does not exist.
ICAO also said directly to aircrew, in its CART guidance:
“Crew members should:
- participate in their national vaccination programmes recognising that vaccination offers personal protection from infection and can assist in recovery of global connectivity;
To protect the health of crew and others, including co-workers, crew members should:
- Participate in their national vaccination programmes recognising that vaccination offers personal protection from infection and can assist in recovery of global connectivity”
ICAO CART Crew Module – Crew Members
“Should” is not “must”. ICAO’s stance here does not in any way justify mandate, which is illegal under international health law due to the perversion of bodily autonomy and the violation of laws and ethics stemming from the Nuremberg Code, which outlaw coercion or force. Therefore, ICAO’s guidance and stance cannot be used to justify or legitimise any ICAO nation state’s particular policy in respect of gene therapy mandates.
Furthermore, at the time ICAO published its above statements, gene therapy performance, efficacy and risk was still not fully known and also being knowingly misrepresented by manufacturers, governments, media and bodies including WHO, CEPI and GAVI as being circa 95% effective.
Here ICAO is also telling individuals to engage in medical treatment for the benefit of others. This is fundamentally at odds with the basic principle of why anyone accepts medical treatment. They weigh personal risk benefit and do it for themselves as an individual, not for the benefit of a third party. Any larger societal benefit is an emergent outcome from, not a primary reason for the individual’s decision. To stress collective benefit could be considered a form of mental pressure or coercion.
CASA and Dr. Manderson’s ICAO deflection falls short
“The International Civil Aviation Organization endorses vaccination against COVID-19 as a core element of a multi-layer risk management strategy for aviation safety and international air transport. This includes vaccination of aviation personnel.”
In using this passage as a reply to the public’s 11 questions around vaccine-induced myocarditis and pericarditis, what is it saying? Effectively:
“ICAO’s endorsement of Covid-19 gene therapies gives top cover and legitimacy to CASA’s Australian regulatory decisions to mandate aircrew. It is ICAO before it is CASA. We want you to believe that ICAO’s endorsement is synonymous with Australia’s mandate and therefore excuses or justifies CASA. CASA has a defence based on consensus stemming from ICAO CART and other ICAO nations.”
None of this is legitimate or true. It is CASA and the Australian government who are responsible for its territory and jurisdiction.
ICAO did not specify “must”. ICAO nations are only subject to a “should” from ICAO, which is not definite.
Dr. Manderson wanted to and has created an aviation environment in which vaccine-induced pilot injury is normalised into an accepted but certain risk. Prior to Covid, no one espousing such a position would have been considered sane because it runs directly against all established aeromedical rules from ICAO down, which have been abandoned in the last two years. All that keeps a vaccine-induced injured pilot away from the controls of an aircraft is luck of timing or their own judgement.
One thing is certain: it is extremely difficult to determine vaccine-induced injury in entirely burned or destroyed corpses. Without evidence, plausible deniability remains. Two 737 MAX crashes shows us that the industry will enable and tolerate critical failures of regulation.
Regulatory design
For any regulator to be able to truly, effectively regulate, it needs two things:
- Competence in the field it regulates that equals or exceeds the competence of those it regulates, including their competence in tricking, misleading, bypassing or side-lining the regulator. In the case of the 737 MAX, no regulator had sufficient competence up against Boeing. In the case of Covid, no regulator has sufficient competence up against WHO/GAVI/CEPI and big pharma.
- Full, unfettered access to those it regulates. The simple fact that aviation regulators depend upon individual pilots’ self-declaration of medical fitness tells you they don’t have access to the sharpest end of aviation’s current pilot health questions. Secondarily, the regulator has not involved itself in the actions of airlines or unions in how Covid policy has manifested in the form of mandates and employment contracts e.g. “no jab, no job” enshrined in contractual terms. In the case of Covid gene therapies, I believe it may be necessary for the regulator to actively search pilots’ records for evidence of undeclared illness or treatment by dosed pilots after any dose. I do not endorse total power to access records for other reasons. Prior to Covid, medical self-declaration was adequate. Covid gene therapies are a specific case.
Finally, regulators must exist totally free of any form of financial dependence upon those they regulate. In no way should a regulator be able to or need to take money from its market, otherwise it is incorrectly financially incentivised.
However, on this final point, let’s compare the UK’s CAA with Australia’s CASA. Compare their annual reports.
The CAA’s income stems almost entirely from charges it levies against those it regulates, so it is directly, existentially financially bound to them.
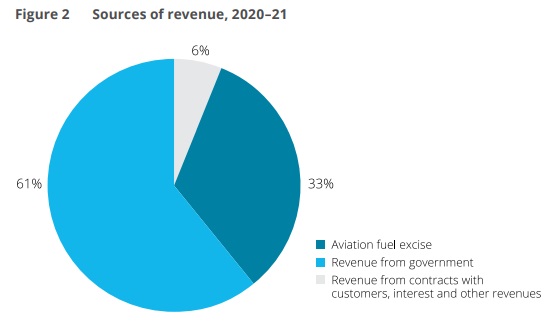
CASA’s income comes predominantly from cash provided by the Australian government. In FY2021 CASA’s:
- expenditure was AUS$193.5;
- income from charges to customers was AUS$12m;
- income from government cash was AUS$128.5m.
Now, assuming the revenue from government provided adequate separation from any vested interest or party e.g. airlines, CASA sort of looks like it meets the last point I stipulate about financial independence from those it regulates.
How then did CASA end up enforcing a worse situation in Australian aviation than in the UK, and ingraining the same risks on a greater scale by making 100% of its operational pilots enter the same, irreversible medical paradigm through mandate?
According to the above, we are left with questions of CASA’s “competence” and “access”. From what I have laid out, I suspect CASA is not medically competent in the context of Covid. I also suspect that it has insufficient access to true information about Covid-19 gene therapies. Therefore, CASA has no option now but to hide from those who question its competence and access.
Conclusion
I posit that the 737 MAX shows aviation is not competently regulated under normal conditions on bread-and-butter issues like “is a plane safe to fly”?
I also posit that Canada and Australia are direct indications that aviation is not competently regulated in the context of Covid.
Were it not for some individual aviators to have themselves critically assessed Covid gene therapies and the wider circumstances of the “pandemic” ICAO and national regulators would have accepted 100% of global aviators being dosed, irreversibly, with medical treatments that it and society at large do not understand. This is synonymous with granting airworthiness certificates to the 737 MAX, which regulators did not understand, except for the fact that the issues in Covid are global and embedded in humans.
Canadian and Australian mandates have robbed consumers of market choice. Consumers in those markets are now forced to accept whatever known and unknown risks now come with being flown by completely dosed aircrew. These two nations have eradicated their control group and diminished safety. The USA would have done the same as would and have others.
Any nation that has failed to critically assess Covid gene therapy in aviators before allowing their use and/or failed to conduct post-dose active monitoring and surveillance – all of them – is not competent in regulating aviation in the context of Covid. This problem goes right to the top and is manifest in ICAO itself, visible in its documentation.
In the case of CASA, to defend one’s own poor actions because of ICAO’s poor actions is inadequate and unacceptable as a defence, akin to arguing that one simply followed orders.




